乳癌的預後因子
乳癌復發的危險因子:
乳癌的復發與每位病人和癌腫瘤的特性息息相關。復發的預後因子包括:
St Gallen 2005/2007對乳癌的復發風險的共識:
低度風險 |
無腋窩淋巴結轉移,且包括下列所有的條件:
1.癌腫瘤大小 ≤2cm,
2.組織學細胞分化Grade 1,
3.無腫瘤週圍的血管侵犯,
4.HER2/neu 基因無過度表現,
5.年齡 ≥35 歲 |
中度風險
|
- 無腋窩淋巴結轉移,且包含至少下列的其中一項:
1.癌腫瘤大小 >2cm,
2.組織學細胞分化Grade 2-3,
3.有腫瘤週圍的血管侵犯,
4.HER2/neu 基因過度表現,
5.年齡 <35 歲
|
- 有1-3顆的淋巴結轉移,但HER2/neu 基因無過度表現
|
高度風險 |
- 有1-3顆的淋且巴結轉移,且HER2/neu 基因過度表現
- 有≥4顆的淋巴結轉移
|
內在的乳癌分子亞型分類法:(St Gallen 2009/2011/2013)進一步加上乳癌腫瘤細胞的基因分析,來為每位乳癌病患『量身訂製』其治療處方的治療指引:
內在的乳癌分子亞型 |
分子生物標記的集合 |
治療的策略 |
Notes on therapy |
Luminal A |
ER (+ve), PR (+ve, ≥20%), HER2 (-ve)
Ki-67: low (IHC: <20%, Gene assay <14%)
Recurrence risk of multi-gene array: low |
Endocrine therapy alone |
Relative indication of cytotoxics:
- High recurrence score (i.e. >25) or high risk of Mammoprint assay
- N ≥ 4 [Minority N(+ve)]
|
Luminal B (HER2 –ve) |
ER (+ve), HER2 (-ve) and at least one of
- Ki-67: high (IHC: ≥20%, Gene assay ≥14%)
- PR (-ve or low <20%)
- Recurrence risk of multi-gene array: high
|
Endocrine ± Cytotoxic therapy |
|
Luminal B (HER2 +ve) |
ER (+ve) and HER2 (+ve)
Any Ki-67
Any PR |
Cytotoxics + anti-HER2 + Endocrine therapy |
|
HER2 (non-luminal) |
ER (−ve), PR (−ve), and HER2 (+ve) |
Cytotoxics + anti-HER2 |
Threshold for anti-HER2 therapy : pT >5 mm or N (+ve) |
Basal-like |
ER (−ve), PR (−ve), HER2 (−ve) |
Cytotoxics |
|
Special histological types |
Endocrine responsive: Cribriform, Tubular, Mucinous carcinomas |
Endocrine therapy |
|
Endocrine nonresponsive: Apocrine, Medullary, Adenoid cystic, Metaplastic carcinomas |
Cytotoxics |
Adenoid cystic carcinoma may not require adjuvant cytotoxics, if N (-ve) |
以內在的乳癌分子亞型來進一步決定手術後輔助性治療的必要性和選擇適當的治療方式。
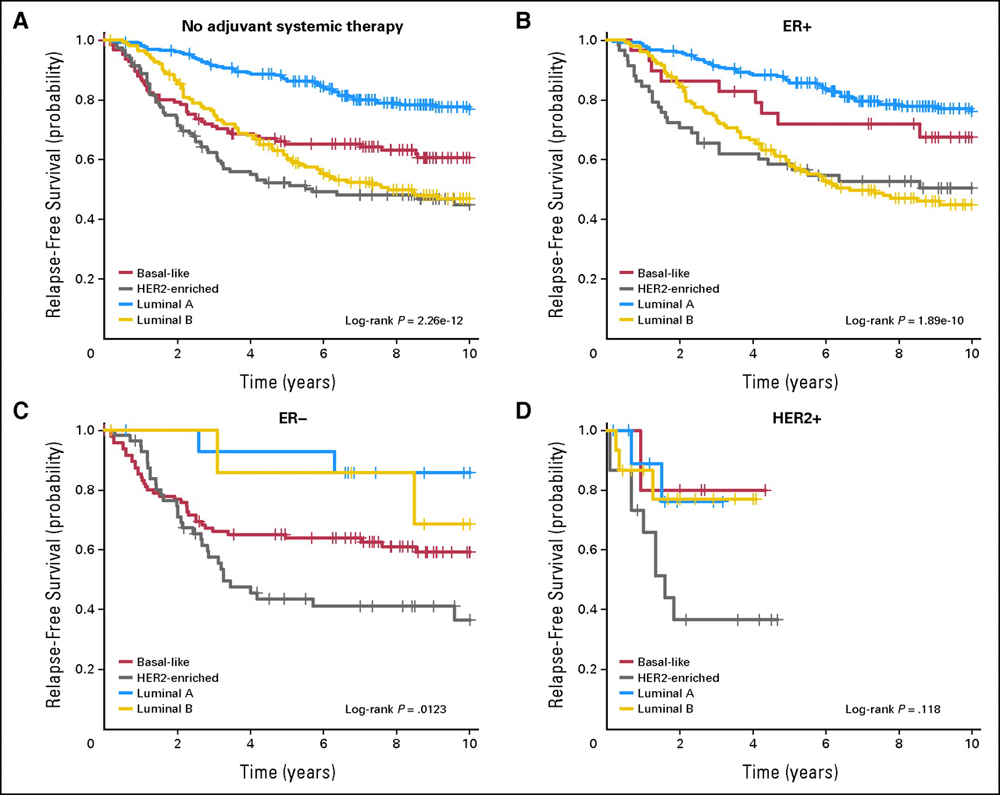
PAM50 intrinsic subtype prognosis for relapse-free survival (RFS). (無淋巴結轉移、未接受術後輔助性全身性治療者,依其內在的乳癌分子亞型,其乳癌復發率的比較圖)(Joel S. Parker et al: J Clin Oncol 2009; 27 (8):1160-1167. © 2009 by American Society of Clinical Oncology)
乳癌基因組測試:
以乳癌腫瘤細胞的多基因組測試來分析未來乳癌復發的風險:如:Oncotype DX-21, PAM50、等。
NSABP-14臨床試驗遠端轉移的復發率,可用Oncotype Dx的復發評分法(recurrence score,RS)分成:
-
RS < 18,低度復發風險(十年復發率6.8%)
-
RS 18-30,中度復發風險(十年復發率14.3%)
-
RS ≥ 31,高度復發風險(十年腹發率30.5%)
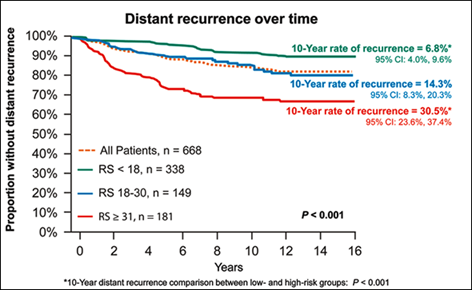
(Soonmyung Paik et al: N Engl J Med 351, 2004; 351:2817-2826) |